► 2021-01-10 Sitrep - 12 reasons things will get much worst!:
In the UK, we're back in a situation a lot like March, when our (so called) government was disastrously inactive in the face of rapid exponential growth of coronavirus infections. They seem to have given up on containing the spread again.
The scariness of inaction spurred me to write my first Covid-19 mega-blog post, initially about exponential transmission. Following up with part 2 and part 3. I looked at all aspects of the Covid situation (and beyond) in the Anglosphere and the world in general. I'll try to revisit some of those topics and my predictions, below, as and when I'm able.
Thankfully there was enough public alarm to instigate action from the bottom up. The much talk about the nature of exponential graphs, thereafter. But it seems we've largely been overlooking the multiplicative nature of case growth again! In different ways, perhaps.
In many ways, the situation is now far worst than March. Despite having 2 vaccines in use and a 3rd approved, way ahead of the absolute most optimistic 12-18 month time frame (that was the expectation 9 months ago). Plus other positive developments, including mandated mask use and refined treatment protocols apparently halving hospital mortality rates.
See Independent SAGE and Christina Pagel for the best briefings on the UK situation. But here's my rundown of why this peak is almost certain to be an order of magnitude worst than the first (in number of deaths, lasting illness, trauma, distress and collateral damage):
(1) More cases and hospitalisations than the April peak- a couple weeks ago (late December 2020) we exceeded the total number of Covid patients during the first outbreak peak (back in April) ~20k. As of 9th Jan we're 50% above that eye-watering level, at ~30k:
... And we're nowhere near peaking yet. The months long period of high transmission (from September school re-openings, onwards) has accumulated many severe cases. There's around 2 weeks delay before the ill become severe enough for hospitalisation. Then often (many) more weeks for recovery, while deaths typically come in at about a month after initial infection.
There were rapid rises in cases in early to mid December [Covid-19 app study], even before the last minute partially aborted Christmas holiday itself. In terms of hospitalisations, we're only just starting to see the impact of that [when I started typing this up on 5th Jan]. With New Year's celebrations then a perfect turbo charger, given the week long (asymptomatic) incubation period between events, multiplying up the effect.
From the graph below: the last 2 week period, with ~78% higher (50k-60k) cases than the fortnight before, hasn't manifested in the hospitalisation figures yet!:
(2) Hospitals exceeding capacity already - in London and the South east. News reports might talk about percentage of available beds filled. But that 'surge capacity' is already expanded well beyond a normal winter! With no more staff, just spread thinner and even more exhausted (with no novelty factor and no end in sight).
The London Nightingale (former Excel Center) isn't even being used for Covid this time, and they can't find the enough regular staff to provide other care there [Metro]. Number of nurses diminish thanks to a decade of real terms pay cuts by the Tories and their jingoistic rejection of workers from over-seas, etc.
ICUs, by name, make intensive use of highly skilled staff and expensive equipment. So it's very hard to expand capacity. The 50% increase, above, is unprecedented. With shell-shocked doctors having no idea what they can do next. 6 days ago some indicated a week before total overwhelm [BBC News].
Expanding capacity is only part of the story - they've also cancelled urgent surgeries (that might need ICU recovery, etc) to accommodate more severe Covid patients [The Guardian]. There's over 3 times more virus cases in ICU than the previous worst winter flu seasons... So far!:
Deaths had been noticeably lower, as a proportion of hospitalisations, so far in this second peak - compare graph below to first one, top. Thanks to refined treatment protocols, knowing which drugs work best, avoiding ventilators where possible in favour of oxygen alone, etc.
But outcomes will swing drastically in the other direction, when hospital capacity is substantially exceeded. For those unable to get any professional treatment, I expect deaths per case will shoot up from <0.5% to closer to 4% plus. Mirroring the scary Chinese stats we say in infographics, at the beginning of the pandemic. The psychological impact of having a loved one(s) slowly dying, unaided, in one's own home... That alone will do terrible lasting harms.
This spectre of masses dying in their homes was first prominently raised by the modelling from Imperial College, released on March 16th, spurring the first lockdown.
Red line (above) is an estimated ICU surge capacity = 8 beds per 100k population (arguably too optimistic). We're currently at around 4 occupied ICU beds per 100k, nationally. But London and the Southeast are at their limit already, with often 300% normal capacity.
It's
valid to look at this early modelling because the numbers of people now
immune from past infections (around 10-15% of population) and the first few vaccinations (<2%) are still
relatively small. Modelling I've previous looked at showed that we
shouldn't expect to see a noticeably reduced rate of spread until we're
very close to herd immunity. Just due to the nature of exponential
transmission.
The blue, 'flattened' curve modelled a (native) R0 of 2.2-2.4 (I think). In theory, we should expect a peak more gradual than that, with mask use and (partial) 'lockdown' mitigating spread. So I 'd guestimate that instead of exceeding ICU capacity by 10 times, it might be closer to ~5 times (if we're relatively lucky). At the moment the R0 value is around 1.1 to 1.3...
(3) The new UK virus variant - Covid-19 B117 has been studied to boost transmission rate by 40-70%, from COGconsotium analysis [Imperial paper]. This is a huge problem, given that our initial lockdown only just contained R0 below 1 (infection rate sustained at the same level). And that was moving into spring, with sunny weather stunting transmission. Adding the new variant's 0.4-0.7 to the first lockdown's 0.6 - 0.7 [Christina Pagel Twitter] takes us to an expected R0 of somewhere between 1.0 to 1.4. I.e. still exponential growth.
This variant doesn't appear to be any more fatal than the original virus. But actually, a more deadly virus would be less dangerous and cause fewer deaths: A flat 50% increase in mortality per case would be preferable verses 50% more transmissions, rapidly multiplying cases out of control [The Atlantic]. A more deadly disease would also be more intuitively scary and likely to motivate more decisive action to stop any spread at greater cost.
During the end of our November 'lockdown' there was a small upturn in cases in London, the East and SE, in line with the emergence of the new variant (graphs below). Possibly showing that, even at a relatively low proportion of cases, it can cause growth during lockdown. Albeit a half-arsed lockdown with schools still open since September. Certainly, country wide tier 4 restrictions alone were warned against, found insufficient in scientist's modelling [The Guardian].
Graphs cropped from [Independent SAGE] presentation (2020-12-29). Roughly same time period covered in each.
Virus mutations happen more rapidly when more people are infected, evolving them in parallel. So the new variant is likely a direct product of our government permitting a high level of transmission in the UK, with its repeated [The Guardian, October] foot dragging on implementing control measures, ignoring their own (and independent) advisors [The Guardian].
And the escalating spread is likely to breed further, dangerous mutations. With concerns that weaker immunity, from partially completed vaccination schedules, could accelerate conditions for evolving vaccine related anti-body resistance (somewhat like anti-biotic resistance).
(4) Weak/no border controlprotections against other new strains- Crazily, we've had a complete lack of testing or screening for infected air passengers landing in the UK. Initial flight controls focused only on China, allowing Spain, alone, to seed around 1/3 of our imported cases [Huffington Post]. Eventually there was 14 day voluntary self-isolation upon returning, cut down to 10 days in December. Very weak.
We're finally introducing a requirement for passengers to get a negative PCR test before flying to the UK [The Independant]. But further details are vague and that alone is unlikely to stop us importing other new virus variants. For example, the strain in South Africa (501Y.V2) which we're worried may have reduced anti-body binding [FT].
(5) Weaker 'Lockdown' - The government's rules are inexplicably laxer, despite the increased danger. More workers are being classed as essential (or maybe just unable to work from home). And so more of their children are at school, too. Plus more students attending, classified as 'at risk'. While nurseries are just plain open, bizarrely excluded from closure. Places of worship, etc.
(5b) Complacent media coverage - Aside from dry numbers and tediously familiar government press conferences, TV news reports have, at most, only been able to show the ambulances queueing up outside London hospitals [ITV News]. So full they've been unable to drop off their patients. Or pick up new ones!
Staff were forbidden from talking to reporters, fairly early on (recent efforts to give them voice here [Twitter]). Access hasn't
been granted for TV cameras in hospitals, other than rare exclusives like this [ITV YouTube]. Even when heard, there, the pleas of the doctors and nurses are so sanitised that they fall flat.
There's no conveyance of the horrendous plight of slowly suffocating for weeks. (Let alone the progressive organ damage and myriad long term symptoms for survivors.) Just a 4 digit number of deaths, that we're mostly perceiving like a surreal weather forecast, telling us we get to go out any time soon. (The 5 dead in the US capital was massive news, 200 times more in hospitals wasn't.)
Also, frustratingly understated use of language, describing hospital ICUs running at 200-300% their normal capacity as under "pressure". No! "A little pressure" is an appropriate euphemism for a nurse to use when administering a jab. Not when thousands are dying per day in overpopulated, understaffed, improvised wards. "Bit of a sticky wicket, what-what."
(5c) Complacent population - even those able to social distance in good comfort may be bored of the stress and limitations. Apathy can be dangerous. There seemed to be a contagious mood of magical thinking, with the end of the year. A very common sentiment that somehow this will mean our problems can just go away, like a new year's resolution. Optimism/normalcy/ostrich cognitive biases, fuelled by talk of vaccinations and hyped up on social media group-think. (And a lack of warning that vaccines won't reduce the need for social distancing for many months.)
From a gif shared widely on social media.
(5d) Very poor adherence to isolation - Only about 18% have been fully self isolating, as part of test & trace [medrxiv via The Guardian]:
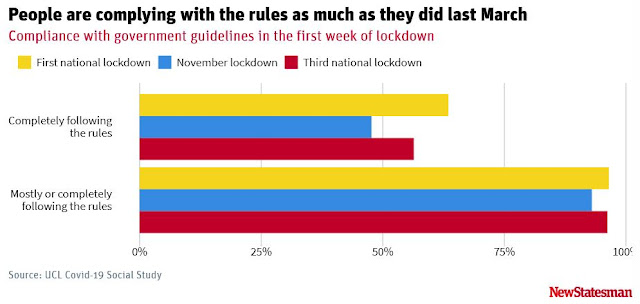
Note: this isn't about "lockdown fatigue" or moral failures! Adherence to general behavioural regulations is still very high, over 90% [BMJ]. Especially amongst students, contrary to sensationalist reports of raves and house parties. (Cognitive selection biases misplacing blame, as I was lamenting back in April.) It's the physical ability to be able to be able to eat, etc, that prevents particularly the economically deprived to stop and just isolate for weeks.
The threat of this imposition, and (£1k to £10k) fines for breaking isolation orders, has led to a rejection of the NHS tracing app and free testing provision, for a huge number of people who can't afford to comply, if found to be infected or have been in contact [iNews].
(5e) Poor financial support - Sunak's financial package offerings have been too small (e.g. [FT]) and grow ever more meagre, with more gaps to fall through. e.g. £4.6Bn lockdown grants [GOV.uk]. Making it impossible for many to eat/pay rent, where they to break from working, etc.
This has been a missed opportunity for launching something like a universal basic income. A cover-all, for those struggling. But anathema to Tory's number one priority of 'labour discipline' (i.e. keeping workers poor and maximally exploitable).
(5f) Disinformation - has grown rapidly in recent years, with these scary times priming people to pay attention to wild claims. There was a video of a mask-less gathering shouting "Covid is a hoax" outside of an overcapacity London hospital, on New Year's Eve, demoralising staff [Matthew Lee, Twitter].
Anti-lockdown Covid (severity) deniers have been platformed by the BBC, for 'balance', with inept arguments put against them. (E.g. focusing on their callousness, rather than the massive concrete factual inaccuracies and oversights in their thinking.)
(5f) Political distractions - Last minute Brexit talks (and a last second not-quite-no-deal with the EU) stole many headlines (and Government attention) in December. It all helped to down out the shouts of scientists (and the public) on the immediate need for stronger Covid measures.
The US presidential transition, too, with
ongoing Trump instigated insanity/insurrection. At best, the full and unequivocal unmasking of the President has lead to more explicit talk of him being sociopath (that I've seen on Twitter). Great is it helps us, over here, to recognise Johnson and his cabinet as
also being dangerously narcissists. Who've explicitly back Trump personally in the past, and with whom we are stuck for another 4
years (short of full nationally collapse and open revolt).
Montage of recent sensational events in the US.
(6) Brexit complications - The previous government's Operation Yellowhammer [Wikipedia] studies investigated the terrible side effects of a 'no deal' Brexit. In its "reasonable worst case" (AKA base scenario) predictions, major disruption to medical supplies (mostly imported) and fresh food were amongst the many expected problems:
Best for Britain [Facebook] summary of report [gov.uk]. My highlights.
Ever evasive of bad optics, our government apparently decided against reevaluating these findings to factor in pandemic problems too. So, as per the new normal, we are flying blind. Unforeseen compounding of problems seems a certainty. Even before the high likelihood of repeat serious winter flooding. (I'm dreading heavy snow travel disruption.)
Technically, the Christmas eve withdrawal agreement [Wikipedia] avoided a no-deal. But it's doubtful many of our MPs, who then rammed it through parliament, have even read the rushed out ~600 page document. I've not seen any headlines claiming to enumerate the most serious shortfalls of this, as yet, since media focus returned to the more pressing Covid crisis. But I get the impression it's not much better than no-deal standard WHO trading terms.
Certainly Northern Ireland's drawn the short end of the stick, in several ways, already having major supermarket shelf shortages [BBC]. Anecdotes of similar all over the UK make me concerned about not getting the fresh fruit, veg and meat that I personally need, due to dietary constraints (and can't stockpile). Worst shortages of these items, than in the early Covid panic buying, were highlighted by industry representatives as a certainty of no-deal [The Grocer]. We may now get to see what it's like to get both issues together.
(7) Crippled by cronyism (and incompetence) - The UK cabinet are disaster capitalists (and their chums). They continue to make a lot of extra money at the vast expense of the nation's misfortunes, often wrought or exacerbated by themselves. For one small example, leader of the commons, Jacob Rees-Mogg, had effectively made £7M on the Brexit referendum outcome by March 2019, from one of his holdings [Channel 4].
Since the pandemic started, the vibe from government (reading between the lines) has been like that of a bunch of corrupt cops, who've casually excused themselves into an OAP couple's home, now gleefully shovelling valuable possessions into bags right in front of them, while their bumbling leader cheerfully chats to one oblivious owner, the other watching impotently outraged and petrified.
I.e. totally shameless and unencumbered ransacking. Cummings was at the centre of it (until ousted by an internal power struggle). But this applies to all of those currently in power, at an unprecedented level, for this country. Producing a tangled web of cronyism (below), from what's been dug up so far by the few news organisations not co-opted by owners who are oligarch, themselves, or with chums in leadership positions. I.e. the BBC's new chairman is Rishi (richest MP) Sunak's ex banking boss [The Mirror]!
They've been awarding billions in government contracts, in secret, with no competitive tender, to mates and former colleges, breaking all sorts of procurement rules in addition [Open Democracy]. Contracts worth tens of millions going to a tiny employment agency, a confectionery wholesaler, £250M through a family office registered in a tax haven, etc [Guardian]. As of June 2020. £32M (75% up front) to "PestFix", a company with only £18k in assets and no experience in supplying the PPE - half the order hadn't turned up, months later. The rest warehoused.
All of this, while frontline staff were dying due to lack of adequate protection (and Matt Hancock appeared to be eating humble pie - just another rodeo clown).
About half of the $22Bn went to politically connected, controversial or inexperienced companies (orange dots). [New York Times, Dec 2020]
As with PPE, test and trace contracts were mostly given to private companies [The Guardian]. Deloitte setting up testing sites in car parks. A network of (often outsourced) national laboratories. Serco taking the tracing phone system, sub-contracting out to others, with inexperienced private staff, who mostly sat doing nothing for the first, badly arranged 3 month contract period. They were significantly less effective than existing, localised public public health workers and infrastructure.
The disconnect between public health and private contractors led to 16'000 tracing contacts falling off an excel spreadsheet being sent to the tracing team [BBC]. And despite ministers (and press) calling the Frankenstein-system "NHS Test and Trace", tests performed by the NHS and PHE couldn't even be input into the tracing app, initially!
It's often been difficult to access and consistently too slow returning tests. The window of opportunity to isolate contacts is very short, in order for the system to stand any chance of achieving it's theoretical 26% reduction in R value, nationally. But almost no tests were even coming back within 24 hours, as of October. (My family had a worrying run-in, in September, with some who thought
they were clear from a routine test, which came back positive a day
later.)
This failed system was reported to have cost us £12Bn, as of October [The Guardian]. More than the entire national budget for General Practices. Rising to £22Bn, as of December 2020 [The Guardian]. More than the total budged of police and fire services combined! Serco repeatedly recieving big new contracts, despite repeated failures [Open Democracy]. Reaching on 2/3rds of contacts (when an estimated 80% of contacts need to isolate for the system to work). Returning only 14% of tests inside 24 hours in mid-October, rising to 38% by November.
Testing turnaround improved into December, despite demand ballooning to 2.4M people in the week 17-23 December. However, tests returned within 24 hours dropped from 61%to 45% [GOV.UK]. A clear sign the system is struggling and will become less functional as our infections continue to soar.
The NHS Covid App, on the Android store, appears to still languishing on fewer than 5M+ downloads (so less than 10M total). I think it it needed to reach well over ~60% of the population to start becoming properly effective (which it's nowhere near). They don't seem to be pushing the app via conferences or advertising, that I've seen (maybe some very targeted?).
It was only rolled out in late September [Wired]. It was delayed for months by gov trying (and predictably failing) to go a unique route, with a centralised data storage system. This was a public confidence nightmare, fuelling fears of sensitive personal tracking information getting into the wrong hands. Still tarnishing the second, functional, decentralised version (based on Google and Apple's APIs), despite this being entirely unlinked to Dominic Cummings. (Who finally left government in November, damage done.)
Data privacy concerns appear to be relevant, still, at least in the context of the big data deals Cummings stuck early on. They gave unprecedented access of NHS datasets to Google, Microsoft and AI firms Faculty (former Vote Leave) and Palantir (Peter Theil's shadowy US private intelligence contractor). Despite initial (false) assurances, it seems our anonymised data could quite possibly be 're-identified' to individuals [Open Democracy].
On September 9th, Johnson trumpeted Operation Moonshot [Wikipedia]. It aimed for 10 million tests per day by 2021, to allow more widespread economic and social re-openings (and Christmas). At a leaked estimated cost of £100Bn! 1/3 the total NHS annual budget! Terrifying. It was quietly dumped the next month (around the time news of vaccine successes came out). It was partially subsumed into Test and Trace, run by (disgraced ex-TalkTalk CEO) Dido Harding.
Education secretary, Gavin Williamson, awarded a contract for kid's laptops to a big Tory donor [The Mirror]. He's also refused cheap/free broadband offers [The Mirror]. Making it harder for disadvantaged children to isolate - receiving no education if locking down at home.
(8) Sabotage - Many Tories have been explicitly working for many years/decades to break up the NHS [Independent, 2016]. Already, much of its more profitable parts have been sold to private companies, on the sly.
So
having the system fully collapse may well be seen as highly desirable,
for many of our ruling party. Enabling swingeing 'reforms', sell-offs,
buying in use of private providers (to re-hire burned out NHS staff at
marginally higher wages, etc). See "How the NHS is being dismantled in 10 easy steps" [Independent, 2017] or "The Dirty War on the NHS", for examples [YouTube].
The
pandemic is also a great cover for Brexit harms which are 100% the
fault of this Brexit (Vote Leave campaign) cabinet. I have been
expecting, for months, that they might cultivate a winter peak to
coincide with EU withdrawal. This makes it impossible to definitively
point a finger at the exact cause of each aspect of the disastrous
situation. Avoiding blame through an excess of chaos. It's hard for us
to conceive of anyone being so callous - again, they are clinically
sociopathic.
(9) Improvised vaccine deployment schedule - Government declared a departure from the 1 month delay between initial and booster injections tested and prescribed by the makers of both vaccines. Instead trying to give as many vulnerable people just 1 dose, over the course of 12 weeks, to spread as much immunity about as possible [GOV.UK].
This sounds very logical. Apart from the initial chaos of cancelling hundreds of thousands of booster appointments. But it's unverified that it will work; keep in mind that the more effect AstraZeneca vaccine 1/2 sized initial dose scheme was found by mistake. So small differences in approach can have unexpectedly big effects.
There's concerns this may increase evolutionary opportunity to incubate a new vaccine resistant variant. As if we'd not given enough to the world, with the more transmissible variant (which has already spread to many countries and is likely to be equally as disastrous elsewhere).
I personally fear that any reduction in the strength of individual immunity, due to altered injection schedules, could be a major issue - if too few people ultimately submit to Covid vaccination, we may fail to reach herd immunity. Which seems increasingly likely...
And the implicit elephant in the room, is that this rush strategy means our public health officials seem to have given up on the idea of being able to control the spread. It's pure damage limitation, protecting the oldest most vulnerable first, when they are the most able to socially distance, unlike young, key workers. If they were pilots, this would be dumping spare fuel and telling the passengers to brace for impact, rather than trying to throttle up and pull up.
Already, it seems to have shot the NHS in the foot, by not prioritising frontline workers. 46'000 workers are now off sick [The Observer]. An estimated 12%, compared to 6% at the peak in April, with up to half of social care staff out in some places, too.
(10) Poor vaccine uptake- Not so long ago, anti-vaxxers were social outliers. But political culture wars against experts and 'the establishment' (from Brexiteers, Trump, etc) have helped promote these beliefs to the mainstream. Along with Russia funded information warfare and meta-conspiracy movements like QAnon exploding on our poorly regulated social media platforms (Facebook particularly). It's a big and hugely important topic that easily merits it's own mega-blog-post.
Some anti-vax groups are apparently quite organised, training members to target their efforts on persuadable friends and family [ITV]. The Center for Countering Digital Hate (CCDH) apparently estimates 5.4M people in UK already follow these beliefs. With 19% growth in followers in 2020 for the top 147 of these misinformation social media accounts [Report].
The [FT] reports a Kantar survey showing 42% in UK will definitely get vaccinated, while a further 33% are less certain (so potentially persuadable either way). And a VCP (Vaccine Confidence Project) study found a 6.4% reduction from the 54% of 4000 people surveyed as "definitely take", after exposure to selected falsehoods [medrxiv].
There's uncertain about the percentage of the population needing to be vaccinated for herd immunity (alone) to fully suppress the spread. FT article says 55%, but before the new variant became news. CCDH states a figure of 82%. Worrying high.
With the transition to Biden and a Democrat controlled US senate, social media platforms are suddenly making more noises about clamping down on dangerous misinformation. But its a huge, unending battle, "on a scale and seriousness of climate change" [Carole Cadwalladr, Twitter]. Trying to reactively counter false claims (screenshot of Twitter ad I saw, below) may backfire, drawing more attention and acting as a confirmation of lies to conspiracy believers. Giving our current, truth allergic, UK government in any degree of control over censorship is also terrifying.
Phone screenshot.
Some are unable to be vaccinated - e.g. immune compromised. And there are legitimate concerns justifying hesitance over vaccinations - the Pfizer-BioNTech vaccine has a warning for possible allergic anaphylaxis, for example.
Personally, with ME/CFS, I'm following a kind of wait and see approach, on the advice of our few disease experts [Health Rising]. Given it is an understudied neuro-immune condition and not even recognised in terms of priority for vaccinations, on the basis of increased susceptibility to symptom effects (which there definitely are, from many community anecdotes).
(11) Winter = no sun = low vit-D: Addressing this with supplements would be relatively cheap, potentially halving severity of any viral outbreaks and slashing mortality from Covid. There's ever-increasing evidence of this [MedCram YouTube].
Another huge opportunity missed by government. An effective daily dose of vitamin-D, offered free to *everyone*, would would reduce all illness and extend healthy lifespans. Instead, I see this [Facebook] advert a week ago. It's now too late to effectively raise people's levels of this critical nutrient/hormone in time for the incoming peak. It's being offered to a tiny sub-population, on an application only basis, so there will be negligible uptake, given most are older age. (Unless they are also mail-shotting everyone.) The offered dosage appears to be only 400IU/day (the defunct meagre daily allowance). A realistic absolute minimum should be more like 1000IU, or 4000IU, to stand best chance of meaningful beneficial effects.
(11b) Other Winter factors- Of course, winter is also worst for spread due to viable virus particles being able to linger on cold (non-porous) surfaces for much, much longer.
People congregating in more enclosed spaces, with outside temperatures too cold to open windows for ventilation. And the UK housing market, dysfunctional for decades, forces many into overcrowded living [The Health Foundation, via The Guardian]. Also exacerbating the mental health burden and impacting (the more poorly paid) ethnic minorities more. Who are already more vulnerable, due to systemic racism and even lower vitamin D levels because of darker skin.
(12) 'Long Covid' - Government and media have laser focused on deaths as virtually the only issue of infections. Which has allowed 'sceptics' to point out that the number of quality adjusted days of life lost is relatively low, given that overwhelmingly older persons die from infection.
They should have been focusing on the huge number of lives already devastated by 'long covid'. Those sick for many weeks, months, or rather failing to recover in most ways. This can happen to anyone, of any age, and might be more motivating to avoid than the abstract 1 in 200 chance of ceasing to exist (about as much as the sanitised daily stats show).
A provisional investigation by the Office for National Statistics [ONS, via Twitter] saw 21% of all Covid cases nationally (not just the hospitalised) were still ill after 5 weeks. 10% still ill at 12 weeks, the longest time interval period in the study! With an estimated 186k Brits currently in that 5-12 week interval of ongoing sickness. That's only up to 22 November, so doesn't include anyone from the (already) bigger second peak!
Earlier in the year [Covid Part 2] we discussed how a Toronto study on the first SARS outbreak saw at least 17% of cases unable to return to work 1 year on [SolveCFS]. But that virus was different, in attacking the lungs and airways far more specifically and immediately severely.
Being part of the ME/CFS community, we know that for many types of viral infections, it's expected that 10% of cases don't properly recover. Instead moving into a Chronic illness state, with diverse symptoms ranging across all organ systems, but most commonly neuro-immune. I think I've seen reference of ~5% or 10% long-covid at 6 months after infection (although no super-concrete big published studies).
A patient led research group surveyed ~4k long covid patients scattered around the world, from 28 days to 6 months of illness [The Guardian]. They each repeated 257 question surveys over many weeks, compiling a big data-set on symptom progression:
The pattern most generally seen is of gradual recovery from respiratory difficulties, but brain fog, neurological symptoms and PEM (post exertional malaise) kicking by the 6th weeks. The most common/defining symptoms of ME/CFS. Certainly, if these persist to 6 months, with no acute illness explanation, long
Covid sufferers would satisfy the traditional criterion for ME/CFS.
Obviously the huge prevalence of these new patients and the similarities have the ME/CFS community engaged - e.g. on this summary discussion thread [Phoenix Rising]. And the attention drawn to this very similar looking cohort with post viral illness looks to be setting free a huge wave of research spending that's likely to help us, too, at least in passing. US congress approved $1.15Bn of NIH spend on long term Covid [Health Rising], when ME/CFS researchers have struggled against repeated rejections for meagre millions, here and there.
There've been many, quite prominent articles about long Covid, raising public awareness and understand by tying it in with ME/CFS too! E.g. from June [The Atlantic]. Pieces from good papers, which show so much understanding and promise, but then leap into the pseudo-science of debunked, but a still sadly influential school of psychologists [The Guardian], now revised of some egregious nonsense. Verses an oddly insightful piece in the [Daily Mail], covering our fight against harmful GET (graded exercise therapy). And even the [BBC] talking about NICE removing the guidance for GET, too.
Yet government briefings don't talk about it; I saw Chris Whitty just barely mention long Covid in passing (sneeze and you'd have missed it). Even if this [C-19 app] study is closer to the mark, on prevalence (13% still ill at 4 weeks, 4.5% at 8 weeks, 2.3% at 12 weeks), I'm expecting 100s of thousand more chronically ill in the UK by next Christmas. Up to a million, if the rate is higher and the virus isn't able to be controlled before most people are vaccinated.
Another enormous scandal, that this problem was known about but glossed over/ignored. Another palpable hit to the nation's productivity too, particularly given younger (and lower paid essential) workers a being thrown under the bus.
• Tentative indications - are that the new B117 variant is controllable, within the UK:
From Christina Pagel here in this Independent SAGE video [YouTube].
We're still waiting for the ONS weekly briefing to more officially confirm this analysis. It's delayed from it's expected Friday 2021-01-15 release, maybe due to difficulties with stats post-New-Year. Public Health England say on [Twitter] that it's with the deaths data. Last week's [ONS] report. Hopefully that will have graphs for the regional breakdown, too, but some numbers were shown here by Independent SAGE [YouTube].
Bad news - cases have plateaued at a level that's just plain unsustainable for the NHS. And have not yet dropped, post-lockdown, in several regions that have little B117. But the great news is that this slight decline in national case numbers comes predominantly from London, the East and South-East, where B117 is already dominant. So it's definitely still possible, in practice, to lower R0 below 1 (from the looks of it).
Phew! Run-away full infection scenario on hold again (for now). Provided this isn't some terribly timed artefact of increased use of less sensitive tests, etc, or government/organisation(s) conveniently mangling data reporting. Maybe I was wrong to extrapolate R0 = 1.1 to 1.4 from naive mathematics. My thinking is that either mask use (shaky as it still is in the UK) is playing a big roll (compared to first lockdown without them)...
Or maybe a large proportion of the increased transmissibility of B117 has been mediated through school children. The government's NERVTAG group were investigating indications of it being more contagious in children [BBC]. Inn which case, closing them could have had an unexpectedly big impact. And higher occupancy (with widened categories of vulnerable and key worker children) would be even more of a concern [BBC]. Let alone an even more damning incitement of government's atrocious mismanagement of their eventual closing [Twitter video].
Good indications that the vaccination program might have actually kicked into full swing, on track for their aim of 2M doses per week [Independent SAGE YouTube]:
But cases are still rising in the most elderly, most at risk age group. A repeat of of the delayed transmission to care-homes during the first wave. But probably more from visiting relatives over Christmas, this time, rather than negligently policy of seeding care-homes from hospital over-spill.
Like many western nations, also with relatively high infection rates, the UK has been prioritising vaccinations to the most vulnerable, starting from the oldest. While this should reduce deaths as a percentage of exposures/infections, it won't actually reduce the burden on ICUs very much because, in practice, the elderly tend to be too frail to be likely to survive ventilators, so are simply moved onto respite care, instead.
So, ICU admissions are massively skewed towards middle and retirement aged patients who are not yet due to have their first jab for weeks. So already overwhelmed ICUs will continue to be more so, as the time delayed impact of Christmas and NYE continues to pile horrendous misery on health professionals, for at least another 2 weeks of slow motion motorway pileup, before deaths even start to plateaux. This situation has been having terrible consequences for weeks already, that are barely being appreciated [Guardian].
Hospitalisations per day 1000 higher than previous peak and may keep spiking upwards for about another week (as far as bed capacity will allow).
I'm expecting the death toll could well peak around 2000 per day by the end of January. The effect of over-full ICUs compounds the number of deaths, too. In normal times, there should be one ICU nurse to each patient, in previous surges 1 to 2 beds, but we're routinely seeing 1 to 4 in many places now. This has a direct effect on survival odds, with over 85% full ICUs, patients die at a rate equivalent to them each being a decade older. Or ~20% higher death rate, currently [BBC].
And this is with a huge proportion of hospital's total capacity turned over exclusively to treat Covid (compared to none before the pandemic, obviously). With most hospitals well over 30% repurposed, up to 66% in one London hospital, that's an enormous flat reduction in overall treatment capacity:
With a system that's been utilised to breaking point during every winter
for about a decade. (A burning problem that I was dismayed would be
sidelined for 3 months by the 2016 Brexit vote, but has now been shoved
aside by that political black hole for closer to 5 years.)
Treatment waiting lists only recently hit an all-time high of 4.46M (previous 4.45M in Nov 2019). With 200k now waiting over 1 year and total numbers treated in November down 27% verses the previous year [ITV]. And it's going to be far worst than November for at least the first quarter of 2021. Personally, I'm 1.5 years into an investigation into unexplained osteoporosis, yet to see a bone specialist who might be able to tell me anything at all about what my initial blood tests might mean.
► 2021-01-18 -Surging inequalities:
• Reason (13) Tory's traditional core priority is sustaining poverty - Another point to add to the 12, up top, about why the UK situation got so bad, dovetailing with: (5e) lack of financial support and (7) crony corruption.
The current government's self serving narcissists successfully took control of the Conservative party by internalising UKIP's toxic fantasies. They are now worst than traditional conservatives, with grift apparently an even higher priority than the pandering to wealth and big business. Closely related to Trumpism eating the GOP, causing dramatic splits recently (following the storming of the capitol, etc). Although it's been far less challenged over here by our news media, due to their overall bias. It's easy to frame Brexit, too, as collateral damage in a battle between robber-baron oligarch disaster-capitalist 'warlord' types, verses the traditional 'house trained' capitalists [George Monbiot, Guardian].
Business as usual conservativism itself has obviously caused great harm too. E.g. contributing enormously to the pain of our health services, via a decade of defunding - reason (8) above. Austerity cuts, brought in by George Osbourne in 2010, gave the UK the slowest GDP recovery in Europe (except for Greece, which was crucified by the bad Euro debt millstone [my blog]).
UK sees its slowest recovery on record, largely thanks to counterproductive austerity [The Independent, 2018].
Cameron's Tories caused enormous misery via their spending cuts, which can probably be blamed for 120k unnecessary deaths from 2010 to 2017 according to one study [BMJ Open, 2017]. Of course it's impossible to attribute such indirect causes definitively [Fact Check]. But a previous study also estimated around 130k from 2012 to 2017 [IPPR, pdf].
So, Tory (mis)rule causing mass deaths is nothing new. Although, Alexander Boris de Pfeffel Johnson and his crew are looking set to match the body count, from a decade of cuts, in under 1 year; their pandemic mismanagement has officially bagged the UK 100k Covid deaths, as of 4 days ago when 1564 were reported in one day [The Mirror].
The most enraging thing is that the entire pretext of government budget balancing was proven a lie. After Theresa May's near election defeat to Corbyn's Labour in 2017 [my pre-election blog], the supposed need for austerity promptly vanished [The Independent, 2017]. Government debt reduction was always a con to excuse slashing spending [The Guardian, 2020].
These days, money is always created from nothing as a promise to repay [Richard Murphy Twitter thread]: Government spends by creating money via it's own bank, that it owns (the Bank of England). Gov debt is essentially just guaranteed savings for the rich (with a low interest rate it can control). Tory governments actually avoid reducing this safe investment pool by reducing their revenues, to offset public spending cuts. Taxes really only redistribute individual wealth & controls inflation. It's essentially unnecessary for financing spending. (I first investigated government debt in 2009 [My Blog].)
Rishi Sunak's mysterious ability to suddenly finance hundreds of billions of pounds of spending [The Times], for furlough schemes, private PPE/testing contracts and further stock market support, etc, has been shamefully glossed over most by most of by the media. Perpetuating public ignorance of a fundamental reality [Positive Money].
We keep hearing how the wealth of billionaires has inflated massively despite the current turmoil [The Guardian]. E.g. world's richest up 27% during the pandemic [BBC]. This was primarily thanks to government central banks (like the US Federal Reserve) pumping trillions into the financial/stock markets via new quantitative easing [FN London]. QE became standard after the 2008 crash and has driven surging inequality in the name of stability for the too-big-to-fail corporations, which must keep growing [The independent, 2018].
In April 2020, the [Bank of England] even announced it would finance the government with direct cash, as opposed to buying it's debt through the bond market. A welcome, progressive move [Positive Money].
Given the arbitrary quantity of financing available to our sovereign government, there's no solid reason to chose to support the markets while getting increasingly stingy with support schemes for the public. When these are essential for people to be able to adhere to Covid self-isolation. (And there spending will in-turn stimulate more spending, unlike supporting the wealth hoarding rich, with minimal trickle down.) Here's Our chancellor lying about the nature of its money [Positive Money]:
• It's the money, stupid! - It's become very clear that pressure from workplaces for employees to keep coming in [Observer] and widespread financial insecurity have been (by far) the main drivers behind excessive population mixing, pitiful self-isolation compliance. See (5d) and (5e), above - I was probably wrong to talk about public complacency (AKA pandemic fatigue) at all, really [BMJ Opinion].
2.4M people in UK experienced destitution in 2019 (many in work), including 555k children, up 50% [Channel 4 Youtube]. So the pandemic has made a bad situation far worst. Insecure, or (newly) self-employed workers, due to no fault of their own, fall entirely between the cracks of the available furlough, Universal Credit and spattering of other support schemes.
"After a year of joblessness, Britons receive average of 17% of their pre-unemployment income compared to 59% in Germany, 54% in Spain or 34% in New Zealand." [FT, via Twitter] Workers in the UK have the worst guaranteed income for sickness or self-isolating, out of all the [OECD] countries:
Patching up this half-arsed mess with more support (or even going properly progressive with a blanket UBI) might actually be relatively cost effective at reducing spread, compared to the increasing billions thrown at the privatised test and trace systems. Especially if usage of/adherence to them remains low. It would act as stimulus, multiplying spending and tax returns.
Yet government is still, on Monday, [BBC] hoping to head off Labour's scheduled debate attempt to have them commit to keeping the £20 'uplift' added to Universal Credit payments, past March. This currently brings a single qualifying claimant up to barely ~£100/week [Money Advice Service].
• A female burden - Acute infection kills more (older) men. Probably more overlooked is the gender split of debilitating 'long Covid', at least twice as common in (younger) women [Daily Mail]. Like there are around 4 times more women with ME/CFS and other chronic inflammatory diseases [ME Research]. Often neglected of research and treatment funding, partly due to the patient demographic.
But lockdowns have also been a disaster for working mothers, having to shoulder most of the burden of school kids suddenly stuck at home, or without daycare [The Guardian]. The majority (71%) were refused furlough, when asking to look after their children. According to a recent survey of 50k mothers:
• Widening education chasm - Distance learning, during lockdown, is profoundly amplifying the relative advantage of school children's family setting. About 3/4s of private school children still had full days of learning, from home, verses 39% at state funded schools [LSE blog].
The contrast between those with their own laptops and good quality
internet access being even more stark. Especially given government's
blundering failures to support these needs. And it's also a nightmare to figure out how to fairly assess grades for progression to further education, particularly.
The Institute for Fiscal Studies (IFS) Deaton Review of Inequalities warned that the educational consequences of the pandemic may be even more worrying than the unprecedented economic impact [BBC].
• Feed our children! - There has been an ongoing battle, with the government, to keep disadvantage/vulnerable children fed, particularly through the summer and then Christmas holidays [BBC]. At least these scandals have been in the public eye. Although that's taken the heroic effort of famous footballer, Marcus Rashford [End Child Food Poverty] via [Twitter]. (Social media now often more fundament than freedom of the press, in getting the ball rolling on important issues.)
Of course, the government privately outsourced contracts to provide the food parcels (without tender). Almost £350M going to Chartwells. Its parent company, Compass Group, chaired by Tory donor, and 2014 government advisory group member, Paul Walsh [Independent]. The world's largest catering company, in 2006, paid a £40m to settle two lawsuits, after allegedly attempting to bribe a UN official for a contract to supply peacekeepers.
There was a similar story with food packages for vulnerable shielders, earlier in 2020. Bidfood and Brakes was reportedly paid almost double the £26 retail value, £44, for the 4.7M boxes provided [Good Law Project]. With contents often inedible, probably discarded as unsuitable from elsewhere in food distribution.
• Authoritarian slide- Our government has an idealogical penchant for suppressing the population, e.g. with stricter laws. Plus it needs to be seen to plausibly be doing *something* to address the continuing high levels of virus transmission. And it won't really address the causes of people piling into regular commutes like in these scenes [Twitter video]. Let alone the less visible daily grind...
So ministers prefer to talk about police getting 'tougher' on rule breakers [Reuters]. Even though various over-reactions have caught media attention, been ridiculed and derided. E.g. two (posh looking) female friends out for a walk were surrounded by police and finned £200 [BBC]. And may have played into the hands of anti-lockdown activists via a supposedly 'staged' arrest of woman for sitting on a bench [The Independent].
It's entirely sensible and proportionate to actually enforce wearing of masks when grocery shopping. And break up odd house parties, etc. But this: "Ms Patel portrayed the strengthened enforcement as an alternative to
introducing still stricter rules than those currently in place..." [FT] is an inappropriate dichotomy. It totally overlooks the excessive number of employers making workers come in and lack of financial ability to comply with existing measures, for many. More fines won't help there.
You just know fines and harassment will quietly impact those whom the
police normally focus a disproportionate amount of time on -
ethnic/black minorities and disadvantaged. E.g. looks like the Met were
twice as likely to fine black people [The Guardian].
Emphasising petty legal enforcements perhaps plays into our national character, as curtain twitching snitches [The Guardian]. Somewhat of a security theatre, compared to the main issues (above).
There's a good argument to say that over-representing rule-breaking,
like this, may have a direct negative effect on compliance [The Guardian].
Or at least moral. So much more of a focus on positive anecdotes about
compliance, despite difficult circumstances, would be more productive
(and emotionally uplifting).
But government (and press barons) want the distraction of the divide and conquer effect, as I talked about at the top of [my 3rd Covid blog]. Social media commenters bristle at headlines like ""Hundreds of incidents" of people ignoring lockdown restrictions in Lancashire have been reported over the weekend, police say." [BBC]. When the top 2 cited infractions are "Three men inside Pub" and guy filming on the street.
Everybody thinks everyone else is the problem [You Gov, via Twitter]
• Stripping protections - We're already seeing confirmation that the Tories will use Brexit to rip into EU protections on worker's rights. Cutting annual holiday down from 5.6 weeks to 4 and extending 48 hour default limit on the working week [FT via Twitter]. Really dumb, given UK's productivity (GDP per person hour worked) has already been struggling. Only Japan is worse (with even an more insane 'work ethic'), while "The average French worker produces more by the end of Thursday than their UK counterpart can in a full week" [FT 2018], with their shorter hours and more time off.
Government still striving to make most workers as powerless, poor and pliable as possible [Ed Milliband in The Guardian]. Labour exploitation makes little sense for a nation with scant manufacturing or resource extraction. But instead much high tech, high skill, high value service and information economy, which increasingly need more better educated and well resourced workers. But are being wrecked by Brexit brain drain and xenophobic repulsion of (settled) migrants.
The Equality and Human Rights Commission has been directed away from prioritising gender and racial equality, towards the government's "levelling up" agenda, focusing on the white working class [The Guardian]. (Who it's unlikely to help much either.) Its political independence was thrown out the window with the appointment of a new head and commissioners, at the end of last year. It's funding had already been cut down from £70M in 2007 to £17M now. It investigated anti-Semitism in the Labour party last year, but paused it's look into Tory party Islamaphobia, pending their own internal investigation, which is overdue with no news.
► 2021-01-20:
• Stripping sovereignty & the NHS - The Conservative majority voted to deprive themselves of the power to scrutinise new trade deals in parliament [Caroline Lucas Twitter]. Taken in the context of US officials insisting upon the NHS being 'on the table' (particularly regarding the pharmaceutical industry), this appears to make further (stealthy) privatisation of public health provision very likely [Independent].
The UK private health sector is already cashing in from the boom in demand stemming from NHS overflowing capacity [Guardian]. In the first wave, up until August, beds were bought for emergency non-Covid treatments, at a total cost to government of £1Bn. But now, there are elective surgeries going ahead (some being paid for by the NHS, one case I know of personally). While negotiations falter for critical care.
• Legal delays - Covid restrictions have impacted the legal process, making trials awkward. But the pandemic itself has caused only a modest effect to a system that was already severely backlogged by budget cuts to police and Crown Prosecution Service [BBC].
The total criminal courts backlog is up 100k, in the last year, to over 457k. They were already dealing with 3-4 year delays for cases of simple theft. With 15% of the prison population comprised of those on remand, awaiting trial. Education provision in prisons cut and Covid outbreak risks heightened.
Victims of serious crimes, too, living for years with crippling anxiety/fear, awaiting trials. Many forced to give up on justice altogether. I'd expect the government to make scary cuts to the quality of the legal process, to speed things up, rather than returning the modest funding needed to enforce a lawful country.
► 2021-01-29 - Contagion dynamics vs testing:
• Dispersion factor, k, is more important than R0 - The average rate of transmission in the population as a whole (or
region) is constantly referenced, in updates about Covid virus spread: Rt, at the present time (as control measures change).
This [The Atlantic] article (from October 2020) points out why k is more important to understand and planning how to maintain a low level of transmission (or eradicate it). A summary that I originally laid out in a Facebook post (at the time):
(1) Sars-Cov-1 and 2 are "overdispersed" (high k value), because roughly 20% of infection cases account for 80% of the onwards spread. Flu has a more homogeneous spread, so only R0 really matters there.
(2) Some people may shed far more Covid viral particles than most do. But environment is also key - indoor, poor ventilation, crowds, loud talking/shouting/singing, no masks, make a big cluster of transmission far more likely. (E.g. "Patient 31" in South Korea caused 5000 known cases in a mega-church cluster outbreak.)
(3)Reverse contact tracing, to identify probable super-spreading events, could thus be 2-3 times more effective than *only* focusing on downstream contacts of a brand new confirmed cases. (As UK's mostly privatised Test and Trace system has been doing, poorly.)
(4) Less precise (but faster/easier/cheaper) tests can be more useful for this tracing method, by getting *all* potential contacts to isolate if just a few positive results indicate there was a cluster event.
(5) South Korea and Japan's successes largely stem from such a focus. Even Sweden remained stricter on banning events over 50 persons (while other EU states relaxed). School children under 16 are unlikely to be super-spreaders because they don't get as sick as adults. (I'm not sure if this may have changed, recently, with the B117 variant that is >30% more virulent.)
(6) The worse hit countries and regions (at the start of 2020) may largely have been unlucky. Just a few early super-spreading events may have accelerated their outbreaks far more rapidly. (A little like tiny quantum fluctuations in the first milliseconds of the big bang got blown up by expansion to the huge variations in the microwave background radiation, shown across the entire sky.) So we should be careful not to draw wrong conclusions from local conditions that may well have been merely incidental.
(7) We should focus on intelligently eliminating conditions for potential super-spreading E.g. (back in late summer) crowded pubs (or restaurants) were far more risky than garden parties with slightly more than the 6 person limit.
• Less sensitive tests can be better - as with point (4), above, mass testing to find spreading events or locations is better done with frequent tests that come back more quickly and can be done en-mass.
PCR has continued to be the standard used for UK Test and Trace. DNA amplification from a nasal/mouth swab. It's the most sensitive, so can theoretically find infections the earliest. But only slightly earlier than significantly less sensitive tests, because infectiousness ramps up so quickly (green shaded curve, below).
But that sensitivity can be unhelpful, for blanket testing, because it will find (and isolate) many more post-infectious cases (the long tail on curve). It's also too expensive to use frequently, or on mass, at all. (It was the vast majority of Test and Trace's £22Bn outlay [The Guardian], at time of article.) And slow to return results, commonly taking 24h (or 48h + in UK) with centralised labs.
Cheap, rapid, insensitive blanket testing can catch more cases. [MinutePhysics, YouTube]
• Project Moonshot - reportedly masterminded by Cummings [The Guardian], since ditched after his departure, was to use 10 million rapid tests per day. Back in September, it was Johnson's big hope for reopening to life as normal, at the start of this year [The Guardian]. That now all rests on vaccinations, because there is no other pandemic exit plan [George Monbiot, The Guardian].
There was talk of the Oxford Nanopore's LamPORE tests (which government ordered in advance) - a faster and more mobile DNA amplification method combined with new, high tech DNA reading. It has just been found to have extremely good sensitivity (~100%) and specificity (~99%), in trials [GOV.UK]. But seems its only being used in a few testing trucks, each able to run 2000 tests per day.
• Lateral Flow Tests (LFTs) - came to the rescue in time for early trials of blanket asymptomatic testing, e.g. in Liverpool, during it's November outbreak, pushed by government ministers [The Guardian]. "Made in China by Biotime Biotechnology for the US company Innova Medical and supplied in the UK and Europe by a micro-company called Tried and Tested." Another suspiciously new and tiny provider, given £800M in government contracts, without tender, so far (the most of any private provider).
The tests look and work like pregnancy test kits (picture below). Internal indicative strips, coated in antibodies, which bind to protein structures of viral particles as they flow past.
They were assessed to have a 95% sensitivity for individuals with high viral loads (the important cases to identify and stop), flagging only 76.8% of all infections [FullFact]. Which could be ideal, for the regime described above (to track back to spreading events). However...
• Dangerously misused tests- The accuracy of the LFTs reduces sharply by experience of user: lab scientists - 79%, trained health workers - 73%, self swabbing - 57.5% [Joint PHE & UoOxford preliminary study].
Despite this, the Medicines and Healthcare products Regulatory Agency (MHRA) has authorised them for home use as part of Test and Trace, in late December [GOV.UK]. Quite possibly under political pressure. The reportedly stated, in private emails, to use them only for finding positive cases, not clearing contacts as Covid-free [The Guardian].
But there's major concerns that home users may be taking negative results to mean they are definitely not infected. E.g. a nursing home outbreak (mentioned in article linked). Also, in the [BMJ] "Government uses lateral flow tests to keep children in schools against regulator’s advice". With daily LFTs of pupils *instead* of isolating contacts of known cases. An dangerous inversion of their ideal use case scenario.
There's controversy over the use of LFTs, with some scientists reportedly retubing criticisms, saying that claims about missing 60% of cases had misinterpreted the data [BBC].
► 2021-02-11 - Vaccination & Immunity Outlook:
On a per-dose basis, the UK has been doing very well with vaccine rollout. Israel has been blazing ahead of everyone, having struck a deal with Pfizer for a priority vaccine supply, in return for access to the country's unparalleled 30 year deep public health database on it's 9M population [npr]. Closely monitoring effects and effectiveness as a kind of over-sized trial. Plus the UK's had tensions with the EU, over their supply issues with Astra Zenica's vaccine [The Guardian]. A part of why they currently lag behind, for now, in addition to their centrally organised purchase scheme and longer safety deliberations.
Despite being quick out of of the blocks, there's currently a long way to go for the UK, on all time scales (1 - short, 2 - medium, 3 - long term):
(1) Reducing the immediate risk of death for the most vulnerable (a month or two) - All developed countries have started with oldest citizens first. UK has already given some protection to most of those who are most likely to die from severe infections (hopefully). This effect against morbidity seems very assured, starting from a couple of weeks or so after first injections [e.g. The Atlantic]. There were no deaths or hospitalisations of any (fully) vaccinated trial participants of all approved vaccines [Eric Feigl-Ding, Twitter]. Another srouce, showing outcomes of control groups, etc, too (Oxford/AstraZeneca too, but we'll look at that in detail further down). "NR" = none reported:
The UK was certainly the most desperately in need of this protection, with the highest case numbers and deaths of any country, in January. But other major European nations (and the US) have been struggling badly through the winter, too. So, for once, there is some justification for national pride, in a (so far) successful vaccination program.
But it's important to note that this success is down to use of existing NHS structures and expertise, unlike government's failure with a lashed together privatatised test and trace system [Anthony Costello, Twitter]. And worryingly, our government has still shown no sign of planning beyond this immediate emergency vaccine push. Unlike the US, where the new Biden administration published a 200 page plan on day 1 [Whitehouse_Gov].
Given that only mass deaths have had the political weight to (belatedly) trigger Johnson to follow SAGE advice, a lack of this irresistable motivation makes a return to mass infections seem likely, with many of his back benchers demanding (premature) re-opening [ITV].
(2) Reducing spread to allow lifting of lockdown and some restrictions (many months) - there's a bewildering array of different stats for the percentage protection of each vaccine, at each dosing stage, time from injection and age group, etc (details to follow).
But there's little very solid, so far, on how much vaccines will reduce onwards transmission, in practice. Illness severity is definitely decreased, and the thinking is that more ill = more contagious. But, for example, the headline number of 67% reduced transmission (from one dose of AstraZeneca) [Guardian] is specically talking only about a reduction in the number *testing* positive.
It's hard to test the effect on real world transmission definitively, until most of an entire population is vaccinated. Asymptomatic infected cases might plausibly be the main contributor to overall spread, where isolation of symptomatic cases is effective. And the number of asymtomptomatics might remain similar after vaccination: while asymptomatics don't test positive even with PCR, would-be severe cases (and deaths) seem shifted down to only moderate symptoms, and moderate down to asymptomatic [In the Pipeline].
At any rate, there's no expectation of vaccinations achieving any noticeable reduction in spread, in the UK, until late spring. (See graphs in next section, Herd immunity, below.) So a release of control measures before then is scary, something that scares this German virologist, scientific advisor [Spiegel International].
(3) Suppressing/eradicating infections in every country, to prevent new strains arising (a couple of years) - we're already seeing, from trials of the additional vaccines now being published, that the South African B1351 variant (and Brazilian) have a significantly increased ability to escape the immune response from past infections of the original virus - total escape in 48%, partial in 90% [African CDC, via Twitter].
While Novavax was 96% effective against the original, that dropped below 90% in a more recent UK trial and to ~60% in South africa, with their newly dominant varients [NY Times, via Twitter]. AstraZeneca's recent effectivness in a small South African trial was reported at (very roughly) 10%, causing it's use to be abandoned there [Guardian].
The
UK's B117 varient has been seen to have aquired the troublesome E484K
mutation (of the SA varient), too, in several documented cases [Eric Feigl-Ding, Twitter]. This suggesting convergent
evolution, with strong selection pressures towards a particularly effective trait. Which might be partially good news, if it remains stuck in this niche, as opposed to finding other ways to evade immunity (for now). But means we must keep domestic cases in decline and fully quarantine against imported varients, to avoid a fresh outbreak here.
So, it's certain that updated vaccines will be needed, by this autumn and in future years, to keep new varients from spreading through even those nations who have been fully immunised. Several manufacturers already started work on tweaks for B1351 and B117 (trivial for the mRNA approaches) and UK government has some agreement in place for production of ongoing updated vaccines [New Scientist]. Fully overcoming this situation is going to take an unprecedentedly rapid and well organised global effort. 'Vaccine nationalism' being counter-productive for every nation, in the long run.
• Herd immunity - Here's a graph showing the percentage of the population that will need to be fully immune (y-axis), verses the R0 of any given pathogen. Because the curve is so steep, to start with, that a small increase in native R0 (no social distancing) has a big effect on the population immunity required. From an R0 of ~2.6 (original SARS-COV-2) to an estimated 4.5 [medRxiv, via Twitter] with the B117 (UK) variant. (R0 4.5 is stated there as a lower estimate, but some talk of 3.9 [The Guardian].) So, we go from >60% to around 80% total population immunity required (to relax all control meassures):
Looked at from a slightly different angle. If the whole population has an average level of immunity, shown for each coloured line (below), it will transform a native R0 (x-axis) to an effective Re (y-axis). With an Re below 1 needed to (gradually) reduce the number of infections (towards die-out):
So, even if *everyone* were vaccinated with (all the doses of) a vaccine that only gives 70% protection (on average), the amount estimated for the AstraZeneca vaccine [medRxiv], it would be impossible to control the a variant, if it's intrinsic R0 is greater than 3.5. In other words, we'd still need extra measures, like masks, distancing, effective test, trace & isolate, etc, to bring the observed R value below 1.
Of course, a significant minority will refuse vaccination and many more are hesitant (e.g. a major problem in France and amongst ethnic minorities who've been wronged/ignored in the past). Also, older people tend to achieve lower levels of immunity. So by starting with the eldest first, we've inadvertently been *minimising* the overall reduction on transmission rate. Especially as retired people are more likely able to socially distance, without the need to go to work/school/etc.
• Infection protection - Immunity the hard way! There have been 3.8M officially confirmed positive tests in the UK [GOV.UK]. But the majority will have gone untested, either asymptomatic, unable or unwilling to go for a test. If we take the 117k deaths (within 60 days of a Covid test) [Twitter], and extrapolate total infections based on a 1% mortality rate, we're probably looking at somewhere in the realm of about 12M infections in the UK infected, so far. About 18% of the population, overall. With a higher percentage for young adults (seen in various demographic breakdowns previously).
Public Health England's SIREN study, published 13 Jan [MedRxiv, via GOV.UK, BBC], saw a number of reinfections (within their 6614 participants) suggesting that first time infections gave approximately 83% immunity, at a median of 5 months after infection. Their preliminary findings also showed that some of those with antibodies still had high viral loads. Which is very suggestive of them being infectious, a second time, even if they are asymptomatic.
Multiplying the ~18% estimated total infections by 83% immunity gives us (very roughly) ~15% total population immunity in the UK. Far more than that given by those who've had both vacine doses, so far (<500k, ~1% [SkyNews]), but still negligable, in terms of slowing spread. Of course there will be an amount of overlap between the vaccine roll-out and those previously infected, increasing as it eventually reaches younger adults, too.
------------------------
> Work in progress:
• Vaccines: their effectiveness is stated against various eventualities - death, severe/moderate infection, symptomatic infection, detectable (asymptomatic) infection. E.g. AstraZeneca appears 70% effective against serious illness, but only 50% effective against asymptomatic infection [medRxiv].
Also with reduced effectiveness against the various variants. NovaVax was recently seen to be 89% effective in the UK, but only 49% effective in South Africa, where the B1351 variant is already dominant [The Atlantic].
At full dose schedule - the vaccines approved in the UK are:
Pfizer-Biontec - Gives >90% protection.
But after just one dose - t
Pfizer-Biontech's vaccine trail data [FDA] briefing, page 27 [via Twitter].
Above: Meassured concentration of protective
antibodies found in older adult's blood at days 1, 21, 28, 35 and 52 after first doses. Trialled amounts of 10ug, 20ug, 30ug, placebo control. Second doses on day 21.
30ug is the dose administered in the UK [GOV.UK], apparently tailored to the weaker immune response of the elderly. Those 18-55 years old saw just as strong protection from 20ug (below). But in either case, the amount of antibodies pressent 3 weeks after a single dose is very low (<10% of final levels). Certainly too low to immediately neutralise a live infection before it can replicate. Although give the body many days/weeks headstart on mounting an effective response.
--- There
was no data for this from the original Oxford Astra-Zeneca trials. Then
an (overhyped and shaky) retrospective analysis of this data was
published claiming 76% efficacy of one dose [UoOxford]. But with very wide error margins [In the Pipeline].
---
► Next up:
• Vaccines & immunity.
• Global situation.
• Virus variant details.
• Vaccines overview.
• David Davis, unlikely Vit-D crusader.
• More on Long-covid and ME/CFS.
• Revisiting my past predictions...
No comments:
Post a Comment
I'm very happy to see comments, but I need to filter out spam. :-)














































No comments:
Post a Comment
I'm very happy to see comments, but I need to filter out spam. :-)